Discussion
This study aimed to compare a meal replacement regimen with lifestyle change as intervention for patients with NASH. The results showed that based on the parameters of interest (i.e., IHL content, body composition, metabolic/biochemical parameters, and anthropometrics) both interventions yielded comparable results specifically in terms of reducing body fat mass, IHL content, and hepatic inflammation.
The reduction of IHL content in this study was more pronounced than in another intervention study using mainly aerobic training programs, with a mobilization of liver fat of 30.2% in the exercise only group and 49.8% in the diet and exercise group[44]. A recent systematic review suggested that an exercise program at 70% VO2max is ideal for mobilizing fat from liver among NAFLD patients[45]. The exercise program used in this study was in accordance with such recommendation and was well tolerated by all of the participants. Studies comparing different exercise programs additive to a dietary intervention demonstrated that the effect of physical activity was minor compared to that of a reduction of caloric intake or change in macronutrients[46-49]. The lifestyle education program used in this study aimed to motivate participants to perform at least 150 min (but preferably 300 min) of moderate-intensity physical activity per week. Participants had to attend two exercise sessions per week, doing sports at an intensity based on the suggested heart rate reflecting 60%-65% VO2max which had been tested individually.
The nutritional counselling encouraged participants to reduce caloric intake and motivated them to engage in sports. Due to this intensive program the reduction in body weight was more pronounced in the LC-G than among the participants of the MR-G. However, metabolic changes and changes in IHL content were comparable.
Participants of the MR-G received instructions on the meal replacement regimen in a group session at the beginning of the study and were further advised individually after 6 wk. Both treatment strategies led to a loss of fat mass while preserving muscle mass, a desirable goal of weight reduction interventions that had been previously described[19]. The increased mean metabolic turnover in the LC-G was about 5.7 MET/wk, corresponding to a caloric increment of 430 kcal/wk. Increasing physical activity is indispensable in a long-term weight control program[50]. In a period of one year these behavioral changes may result in a 3.4 kg loss in body weight. However, it has been shown that a dietary intervention has long-term effects in liver fat and metabolism despite body weight regain[51].
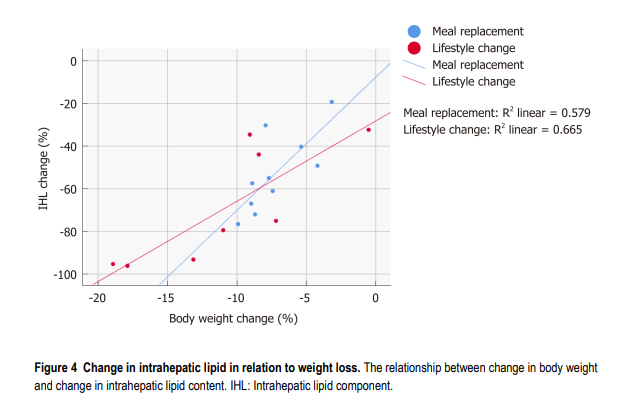
Both groups showed a reduction in cholesterol and triglycerides, as well as an increase in HDL-cholesterol - however, only the decrease in triglycerides in the MR-G was significant. Soy protein with intact isoflavones may decrease total cholesterol, LDL-cholesterol and triacylglycerols and increase HDL-cholesterol[52,53], mimicking the effects of exercise on lipid parameters. The protein content of the nutrition appeared to have a distinct effect on liver fat. An isocaloric protein rich diet, high in animal or plant protein, is able to reduce liver fat by 36%-48%[54]. In terms of body weight change, the MR-G lost more IHL content per loss of body weight than the LC-G. Furthermore, the main weight reduction in the LC-G was initiated through caloric restriction, thus this might have influenced the results. However, physical exercise may lead to a decrease in the intramyocellular lipid content that has been linked to insulin sensitivity[49].
In this study, fasting glucose levels and HbA1c levels decreased similarly in both groups, thus both interventions seemed to be equally effective in improving insulin sensitivity. As NASH is associated with cardiovascular morbidity and mortality[55-58], in addition to an improved glucose tolerance, an improvement in physical fitness and muscular performance is supposed to be beneficial. Expectedly, physical fitness was improved only in the LC-G.
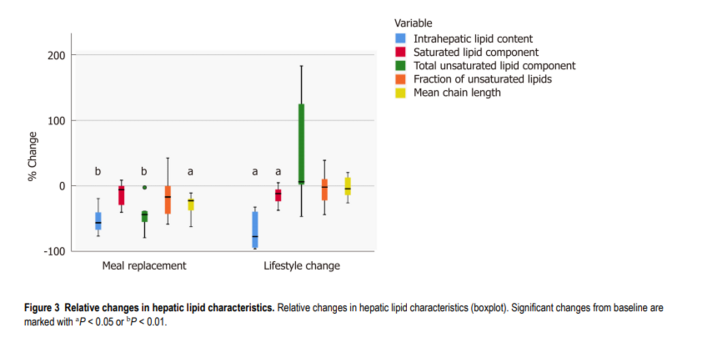
The IHL content was quantified by MRS. With this technique not only the amount of hepatic lipids can be determined with high accuracy[59] but also the mean chain length and percentage of saturated as well as unsaturated lipids may be estimated. However, it should be noted that the calculation of these lipid composition parameters is subject to systematic errors mainly arising from different T2 relaxation of the underlying resonances which cannot be corrected. Therefore, the values calculated in this study should not be regarded as absolute quantities but rather as correlates of the corresponding parameters. With both interventions the IHL content was reduced by more than 50%. The higher reduction in the LC-G was due to a higher extent in body weight reduction in this group. The quality of IHL was more influenced by the meal replacement. In this group the total unsaturated lipid component decreased significantly as did the mean chain length.
A comparable reduction in liver fat was seen in a subgroup of adults with type 2 diabetes examined in the Look AHEAD trial (-50,8% in the lifestyle intervention group)[60] and in patients with NAFLD after gastric banding surgery (-50%)[61]. An exercise intervention in patients with NAFLD led to a weight reduction of -2.5 kg and a change in intrahepatic triglyceride content of 48%[62]. Other interventions have not reduced liver fat content by a similar percentage[7,44,48,55]. An aerobic exercise training that did not lead to a change in BMI led to a decrease in the IHL content of 10.3% ± 4.6%[44], while the combination of aerobic exercise and resistance training led to a reduction of IHL content of 16% ± 24%[63]. Four weeks of aerobic cycling exercise program which significantly reduced visceral adipose tissue volume by 12% without changing BMI was able to decrease IHL by 21%[7].
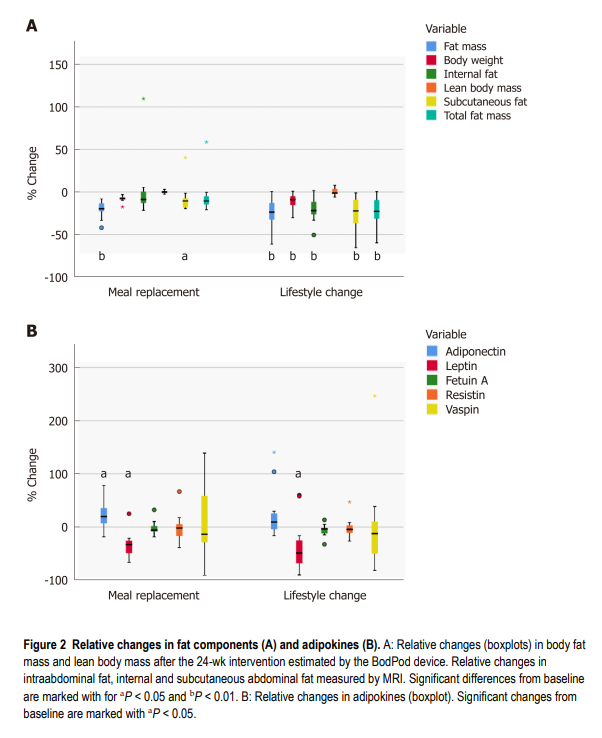
The adipokines showed comparable changes in both groups. There was a marked decrease in leptin with both interventions while adiponectin, vaspin, resistin, and fetuin A showed no significant changes over the 24-wk period. Leptin correlates with severity of steatosis and BMI[64], while fetuin A expression is more prominent in NASH[65]. Both showed no significant changes in both interventions. However, the relative changes in leptin and fetuin A were correlated to the changes in saturated lipid component in the LC-G. Likewise, the study demonstrated no significant changes in the levels of resistin, which is linked to abdominal adiposity and elevated triglycerides[29]. Vaspin which is associated to obesity and insulin resistance[28] also showed no significant changes. In contrast, there is a weak correlation to changes in saturated and unsaturated lipid components. It can be concluded that not only the IHL component is of importance, but also the proportion of saturated and unsaturated lipids since these correlate to adipokines. This may explain why some authors report similar levels among NASH patients and controls in contrast to others reporting higher levels among NAFLD patients[66].
The intervention-induced mobilization of intrahepatic fat was different in both groups. With a soy-based meal replacement, saturated and unsaturated lipids were reduced in a comparable amount, whereas lifestyle intervention preferentially led to a loss of saturated liver fat. Furthermore, the mean chain length was markedly reduced only in the MR-G. The changes in the adipokines adiponectin and leptin were correlated to changes in saturated and unsaturated intrahepatic fats, both in the opposite manner. The alterations of liver fat quality were different between both groups, as shown in Figure 3. The results of this study demonstrate that interventions may not only lead to a reduction of liver fat, but also to a change of liver fat quality. Several studies proved a beneficial effect of a dietary approach to an increase in intrahepatic unsaturated fat in NASH. In a model of rats with NASH the administration of omega-3 polyunsaturated fatty acids improved the spectrum of adipokines significantly[67]. In patients with fatty liver disease the hepatic fat content was associated with high energy, high fat, and high saturated fat intake[68]. By a modulation of fat consumption with increased intake of omega-3 polyunsaturated fatty acids in NASH adipokines and markers of hepatic inflammation were changed positively[69]. On the other hand, hepatic n-3 polyunsaturated fatty acid depletion promotes steatosis and insulin resistance in mice and humans[70]. Therefore, a non-invasive analysis of hepatic fat quality may identify a group of NASH patients which could benefit most from supplementation.
In terms of study limitations, the gold standard of assessing hepatic inflammation and fibrosis, as well as lipid content is still histopathological analysis. Presently, 1H-MRI analysis is a standard method to quantify hepatic steatosis. However, it is not able to assess inflammation or fibrosis. For evaluating fibrosis the non-invasive Fibroscan is conventionally used. In the present study, the focus was on changes in body composition and related IHL changes. Moreover, it was not possible to ascertain whether the caloric restriction in the MR-Group or a specific effect of the soy-yogurt-honey preparation led to the different composition of liver fat. However, our study once more confirmed, that with a supplementation of high quality proteins a significant weight reduction without loss of muscle mass is achievable. Finally, the study sample was not large enough to analyze study participant subgroups (i.e., sex and age groups). The small sample size of the study was partly determined by the exclusion criteria, ruling out patients taking hormonal replacement/substitution, anti-diabetic drugs or lipid-lowering drugs.
The comparability of both intervention strategies suggests the need for further studies to evaluate the course of hepatic fibrosis in patients with NASH succeeding in a weight reduction program. For physicians managing NASH patients, this study suggests that a soy protein-based meal replacement therapy may be an alternative to a therapeutic lifestyle change, considering the patient’s demands and circumstances. The different changes in hepatic lipid characteristics in each intervention need to be further evaluated.
In conclusion, comprehensive lifestyle intervention and meal replacement regimen had comparable effects in terms of weight reduction, body and liver fat content, and markers of hepatic inflammation among patients with NASH. Lifestyle change may be the ideal approach associated with improved physical fitness and muscular performance, while meal replacement could be an alternative intervention depending on patient’s characteristics, level of motivation, and other life circumstances. The two described approaches changed the amount and quality of IHL content with regard to fatty acid chain length and ratio of saturated/unsaturated lipids. The impact of these findings needs further investigation.