Methods
Seventy-six women were enrolled in this 12 month intervention. Inclusion criteria: Female gender, age between 18 and 75 years, BMI between 27 and 35 and absence of contraindications to exercise. All subjects completed a comprehensive medical examination and routine blood tests. Subjects were excluded if they had diabetes mellitus type II, taking lipid-lowering drugs or medications that affected body weight. 22 participants were pre-menopausal, 50 were classified postmenopausal. Classification of menopause was performed by anamnesis and analysis of LH, FSH and estradiol. If FSH and LH were higher than 20 IU/ml and estradiol < 30 pmol/l, participants were classified as postmenopausal. Metabolic syndrome was diagnosed according to the NCEP ATP III criteria [12].
Written informed consent was given by all subjects; the study protocol was approved by the ethical committee of the University of Freiburg.
The study was divided into two phases; the first 6 month was designated as the active intensive intervention period where subjects had to change their dietary behaviour and increase physical activity. In the following 6 month participants were encouraged to continue these lifestyle changes however they did so without study staff supervision.
Diet
Subjects were instructed to replace two daily meals with soy-yoghurt honey drink (Almased® : amount per serving: calories 180 kcal, total fat 1.5 g, carbohydrates 16 g, protein 25 g, cholesterol 0 g) for the first 6 weeks, followed by the replacement of one daily meal for the next 18 weeks. After this period, subjects were free to use the meal replacement for the rest of the study. During the study, participants were instructed to limit fat intake to not exceed 60 g/d. Subjects were instructed during two face-to face counseling sessions and were given educational pamphlets further detailing how to improve dietary behaviour. The regimen contained about 1000 kcal/d during the first 6 weeks and 1500 kcal/d for the next 18 weeks. Participants monitored their dietary intake using 3-day food records at the beginning of the study and at 3 and 6 months.
Physical activity
Subjects attended twice weekly 60 minute endurance physical activity sessions during the first six months. The activity sessions were supervised by a trained exercise counsellor and lasted for 6 months. Compliance was assessed by participant attendance at the sessions. Adherence was good as participants attended more than 80% of the sessions. The training program consisted of mainly aerobic or endurance type activities such as pulse-controlled walking and team sports.
Data collected at baseline and 12 months were body weight, fat mass, fat free mass, hip and waist circumference, blood pressure and blood collection for serum lipids, plasma glucose, insulin, leptin, cortisol and C-reactive protein.
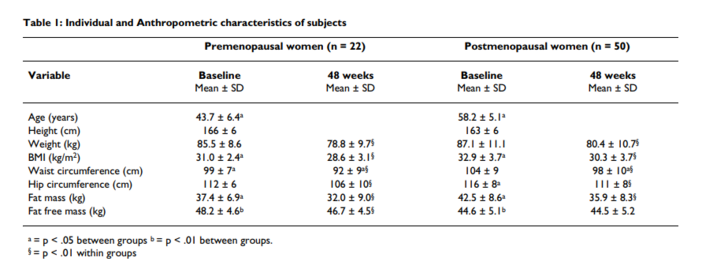
Anthropometrics
Height was measured while subjects were barefoot. Weight was measured using a digital scale, with the participants wearing light clothing or underwear, and was recorded to the nearest 0.01 kg. BMI was calculated as weight divided by height squared (kg/m2). Waist circumference was measured at the level midway between the lowest rib margin and the iliac crest to the nearest 0.5 cm. For body composition, the technique of the air displacement plethysmography was used (Bod Pod®) [13].
Clinical measurements
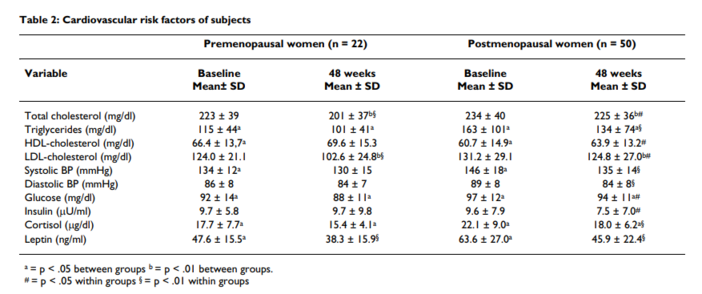
Blood pressure was measured three times in the right arm in the sitting position using a standard mercury sphygmomanometer, with at least 5 minutes rest between measurements. Korotkoff's phases I and V sounds were recorded for systolic (BPsys) and diastolic (BPdia) blood pressure, respectively.
Serum analyses
Cortisol, Insulin and Leptin were measured by commercially availably ELISA-tests (DSL Deutschland GmbH, Sinsheim, Germany). All other laboratory analyses were done in the central laboratory of the University hospital using clinical routine methods.
Statistical methods
Normality of all variables was tested before statistical analyses using the Kolmogorov-Smirnov test procedure. Testing for changes between examination at baseline and at examination after 48 weeks was done by paired sample T-test. The two sample T-test was used to establish significant differences between the two groups at both examinations. All P values were two-sided and a P value of 0.05 or less was considered to indicate statistical significance. Analysis was conducted with the use of SPSS software (version 13.0).