Methods
For effective weight loss, it is absolutely essential to combine measures for changes in nutrition, physical activity, and behavior (4, 5, 6). In keeping with this principle, M.O.B.I.L.I.S. presents individual ways to live a health conscious life. The objective is to achieve a lifestyle with energy balance and improved healthy living skills.
M.O.B.I.L.I.S. is based on the results and experience of the institutions for sports medicine which initiated it and incorporates strategies from behavioral psychology as an essential and original component (7). The most important factor for successful weight loss is the acceptance of the chosen change in behavior and the compliance this leads to. Specific questions of nutrition and exercise tend to be of secondary importance (7, 8). The four central themes are exercise/sport, psychology/instruction, nutrition, and medicine. These are communicated to the group in 20 theoretical and 35 practical units. There are different phases in a defined program calendar for each group. These are distributed over a period of 12 months: a seven-week starting phase, a 17-week weight reduction phase, and a six-month stabilization phase.
Under the leadership of a sports teacher or sports scientist, the participants meet once or twice a week, by turns outside (whatever the weather) and in a hall, to gain sporting experience within the group. The emphasis is on various types of endurance training, such as power walking or Nordic walking, as well as specific exercises to strengthen the musculature and for coordination and relaxation. With the help of the 50+50 point program (specially developed for M.O.B.I.L.I.S.), the participants learn how to implement the listed activities within their everyday lives. The theme of changes in behavior is discussed with a psychologist or teacher in 10 group meetings. Each meeting concentrates on a special group of themes. The participants are given theoretical information and instructed to solve written or oral problems. The volunteers are also called on to continue with specific tasks in their daily life related to behavioral modification and to document progress.
The nutritional section contains three group meetings, one practical meeting and two question and answer sessions; these are led by a dietary assistant or nutritional scientist. Rather than strict diet plans or rigid nutritional restrictions, M.O.B.I.L.I.S. emphasizes orientation towards the correct selection of foods. The most important recommendations are low fat, carbohydrate consciousness, and high protein nutrition. Based on the example of the M.O.B.I.L.I.S. pyramid, concrete recommendations are given for diet which supports fitness and their implementation is practiced. The individual components (behavior, exercise, and nutrition) have already been described in detail in previous publications (7, 9).
In accordance with the guidelines of the German Obesity Society (Deutsche Adipositas Gesellschaft, DAG) (10), the objectives of this program are to reduce weight and to improve the risk factors, health behavior, and quality of life. To achieve this, a trained interdisciplinary team supports the participants in the course of a year to prepare personal health concepts and objectives and to integrate these into normal daily life. This team consists of sports scientists and psychologists/teachers with experience of working with groups, as well as certified nutritional scientists and doctors.
A local training group includes both men and women. The group should include between 15 and 18 people. Formation of new groups is announced in good time over the local media, as well as on the M.O.B.I.L.I.S. homepage (www.mobilis-programm.de). Adults are enrolled with BMI from 30 to 40 kg/m2 and with a comorbidity associated with obesity, such as hypertension, insulin resistance and/or dyslipoproteinemia. There is no age limit in principle. However, the participants must still be capable of exercise, i.e. asymptomatic performance of at least one Watt per kg body weight and adequate motoric competence. For the exercise practice, they must be capable of taking part in walking sports, such as power walking and Nordic walking.
Exclusion criteria are:
-
Contraindications to physical exertion (11) and weight reduction or calorie restriction (10)
-
Type 1 diabetes
-
Liver and kidney damage with the indication for restricted protein intake
-
Psychiatric diseases and eating disorders (bulimia, bulimia nervosa, binge eating disorder)
-
Intake of anti-obesity drugs
-
Status after malignant disease with freedom from disease of less than five years.
As of 1 January 2008, the total costs per participant are 785 euros for 12 months of group care. As a result of an overall agreement with the Barmer Health Insurance Fund, costs can be reimbursed as a lump sum, in accordance with Article 43 No. 2 of the SGB V [Social Security Code V], with a personal contribution of 100 euros. M.O.B.I.L.I.S. is also open to people insured by other health insurance funds. Thus the conditions have been created which would permit implementation of a program for obesity treatment throughout Germany under standard conditions. M.O.B.I.L.I.S. is administered through a charitable society and pursues no commercial interests of any sort. The planning of the program is also independent of the interests of third parties.
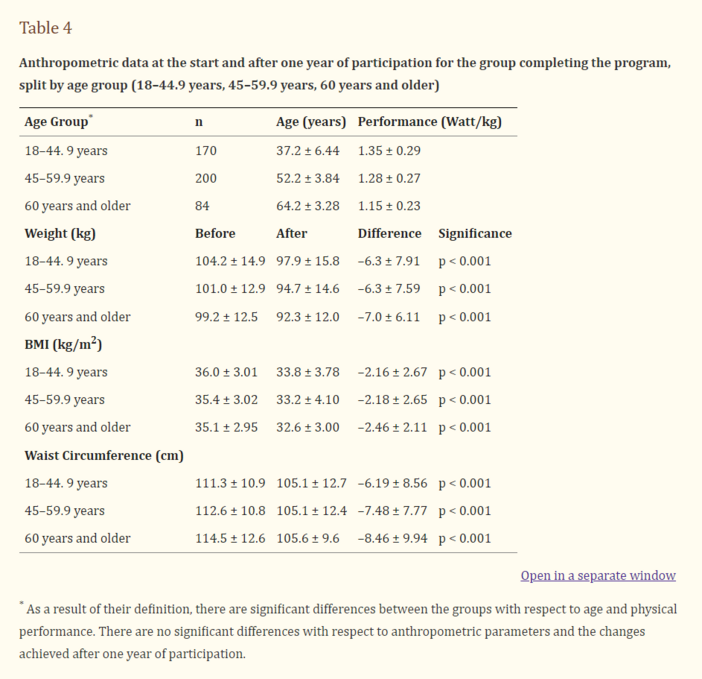
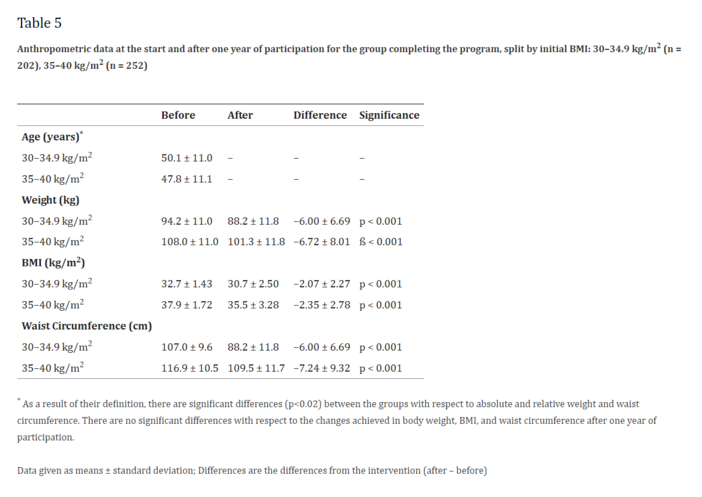
The results and changes are followed during the course of the program. This is based on Case Report Forms (CRFs), kept by a doctor, and with defined examination time points (at the start, after six months and after 12 months), as well as with a questionnaire on activity and quality of life (Freiburg Questionnaire on Leisure Time Activity [Freiburger Fragebogen zur Freizeitaktivität]; Questionnaire on State of Health [Fragebogen zum Gesundheitszustand], SF 36, Hogrefer Verlag, Göttingen). The documentation covers not only changes in weight, but also reduction in health risk factors and changes in health behavior (exercise and nutrition) and in the quality of life. The participant’s weight and waist circumference are measured by standardized methods in the team doctor’s practice. It is possible to take meal replacements as a supportive nutritional measure (10) – such as a clinically tested soy-milk-honey product (12). This was also queried by the team doctor and documented in the CRF. The team manager also documented presence at the training units. In addition, the questionnaires recorded participant satisfaction in the individual phases of the training program, which were then evaluated with the balance score card system. These data are evaluated soon after collection and support continual adaptation and improvement in the training program.
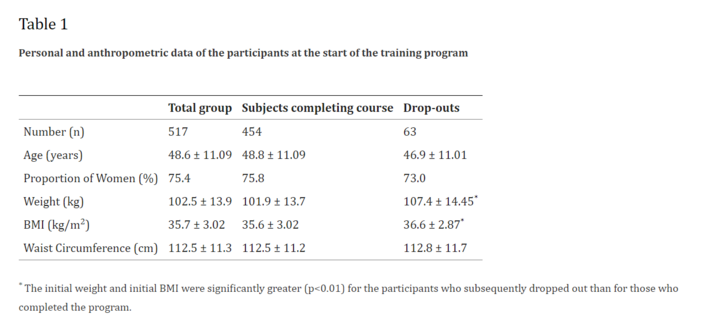
There are now M.O.B.I.L.I.S. teams at about 100 sites, organized by a central office. Between 13 January 2004 and 31 December 2006, 1412 obese adults started the M.O.B.I.L.I.S. program and 517 have already completed it. Eminent politicians have served as "godfathers" for M.O.B.I.L.I.S. in their home towns or electoral districts and have served as patrons or advocates of the project. This has won high general esteem for the program. Details of the program’s organization can be found on the M.O.B.I.L.I.S. homepage (www.mobilis-programm.de), which is updated daily.
All participants take part freely in the training program and the subsequent data analysis, after giving their written consent. They receive no fees for participation or success. The program is performed with the agreement of the Ethics Committee of the Faculty of Medicine at Freiburg University.
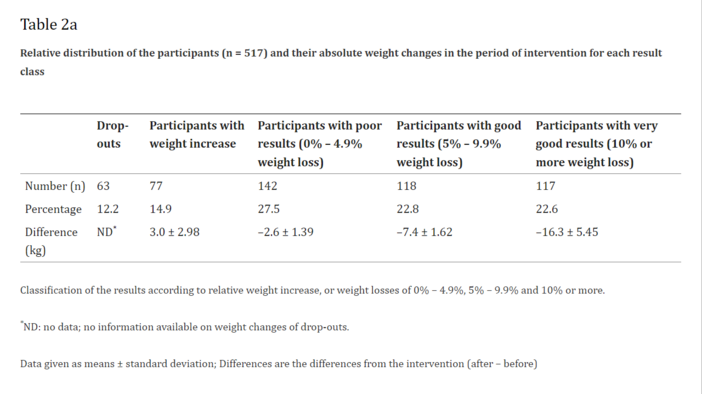
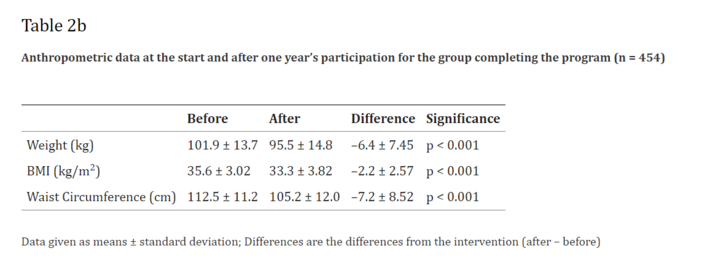
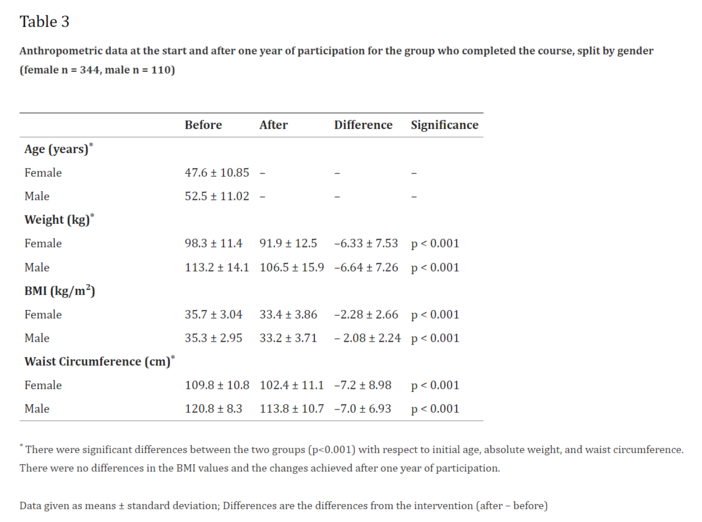
SPSS 13.0 was used for the statistical evaluation. The Wilcoxon test for paired samples was used for the intraindividual comparison between the status before and after intervention. Variance analysis was performed to establish whether there were significant differences between the subgroups with respect to the differences before and after intervention.